
LIVER SURGERY REVISITED
Development of modern liver surgery
Sir
H P Grewal, in his Feb 2 Commentary,1 gives a comprehensive historical account of the development of modern liver surgery and liver transplantation. He repeats most of what has been written on the subject but some facts have never been told.
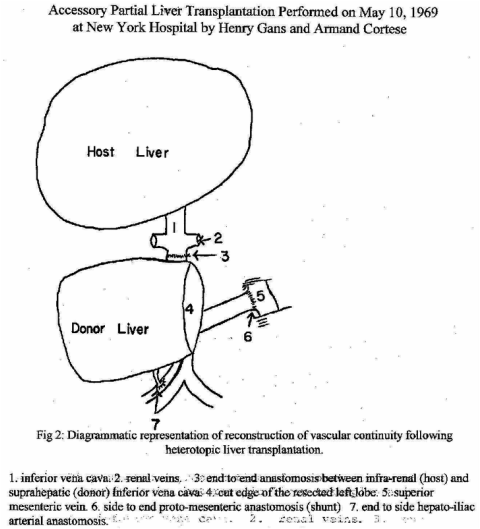
In 1969, Cortese, Richter, Mori, and I, with Minick as pathologist, at New York Hospital-Cornell Medical Center, did two partial liver transplants. In May of that year, in a woman aged 24 years who had terminal liver failure, we ran into unexpected difficulties after finding that, despite massive ascites, her abdominal cavity was not large enough to accommodate a second liver. Had we proceeded, the resulting tension would have severely interfered with her circulation and respiration. Therefore, I resected the donor liver's left lobe while the organ was being perfused in a steel pan, as outlined 15 years earlier.2 The operation was successful.
3 months later, we felt sufficiently confident to again resect the left lobe of the donor liver, obtained from a boy aged 6 years and intended for an infant aged 20 months with biliary atresia. The resection eliminated the discrepancy in liver size. When we did these pan-lobectomies, no available text that we knew of described how to deal with this difficulty.
We submitted a report on our initial case to two surgery journals, but it was rejected. The reasons given were that the two unusual features were heterotopic placement of the graft and hepatic lobectomy to reduce liver mass. They claimed heterotopic placement of the graft had been studied extensively in the laboratory and reported clinically, and that no new information was provided. The resection of a liver lobe to provide space in the abdomen was deemed a trivial contribution of only technical interest. This rejection came at a time when the number of transplant cases outside Denver, CO, could almost be counted on the fingers of one hand.
When attempts at normal publication proved futile, we sent the report to the newly established American College of Surgeons/ National Institutes of Health Organ Transplatation Registry.3 Although I have made brief references to it several times, to date no official report of it is on record. Consequently, Bismuth and Houssin4 are generally credited for having been the first to do this kind of procedure after they applied it in a boy aged 10 years with Byler's disease. In their report, they referred to a case by Fortner and colleagues,5 who published the idea.
It is interesting and gratifying to learn after all those years that our idea has ultimately progressed to the split or partial liver transplants that use liver lobes and segments from living donors. That, to me, seems certainly to be a very worthwhile extension of an idea once deemed uninteresting and trivial, and not sufficiently new to warrant publication.
Henry Gans
A Certain Ambiance, Art and Antiques, 522 Colorado Avenue, Stuart, FL 34994, USA
References
1 Grewal HP. Impact of surgical innovation on liver transplantation. Lancet 2002; 359: 368-370.
2 Gans H. Introduction to hepatic surgery. New York: Elsevier, 1955.
3 American Cancer Society and US National Institutes of Health.. ACS/NIH organ transplant registry: first scientific report. JAMA 1971; 217: 1520-1529.
4 Bismuth H, Houssin D. Reduced-size orthotopic liver graft in hepatic transplantation in children. Surgery 1984; 95: 367-370.
5 Fortner JG, Yeh SD, Kim DK, Shiu MH, Kinne DW. The case for and technique of heterotopic liver grafting. Transpl Proc 1979; 11: 269-275.
___________________________________________________________________________________________
THE LANCET · Vol 360 · September 7, 2002 · www.thelancet.com
The patients portal vein was tied off so that all portal vein blood passed through the donor liver. (according to a procedure previously reported by E Bengoechea-Gonzalez, Y Akwane and K Reemtsma: “Experimental Auxillary Liver Transplantation”, Arch Surg 94 (1967):1).
Fortner’s claim (expressed in his NY Time’s obituary) that he was the first to transplant heterotopically a partial liver (heterotopic split-liver transplant) remains unsubstantiated.
In 1977 he reported (in Transplantl Proc 9:(1977):217) that his group, consisting of Fortner JG, Kim DK, Shin MH, Yeh SDJ, Howland WS and Beattie EJ, had transplanted 7 patients with an auxiliary liver. Only one patient had a partial transplant. In this patient only the left lobe was transplanted after the right lobe, while perfused in a steel pan, was resected.
At the time of their report that patient had survived 4 years, dating the surgery to 1972 or 1973, long after 1969 when we did our two cases that will be reported in my memoir: Living Surgical History.
In 1977 he reported (in Transplantl Proc 9:(1977):217) that his group, consisting of Fortner JG, Kim DK, Shin MH, Yeh SDJ, Howland WS and Beattie EJ, had transplanted 7 patients with an auxiliary liver. Only one patient had a partial transplant. In this patient only the left lobe was transplanted after the right lobe, while perfused in a steel pan, was resected.
At the time of their report that patient had survived 4 years, dating the surgery to 1972 or 1973, long after 1969 when we did our two cases that will be reported in my memoir: Living Surgical History.